If your child has autism, speech delay, or developmental regression, and they have not made progress despite therapy, you should consider one important and often overlooked cause:
Folate Receptor Autoantibodies (FRAA)
This condition can lead to a hidden folate deficiency in the brain, even when standard blood tests show normal results.
Understanding this can reveal a new and effective treatment approach.
What Are Folate Receptor Autoantibodies?
Folate (Vitamin B9) is essential for:
– Brain development
– Speech and language processing
– Neurotransmitter production
– DNA synthesis and repair
– Methylation, which is important for brain function
Folate must cross the blood-brain barrier using a specific transporter called: Folate Receptor Alpha (FRα)
In some children, the immune system mistakenly produces antibodies against this receptor.
These are known as:
Folate Receptor Autoantibodies (FRAA)
What Happens When These Antibodies Are Present?
These antibodies:
– Block folate entry into the brain
– Decrease folate availability to brain cells
– Cause Cerebral Folate Deficiency (CFD)
An important point:
Even if blood folate levels are normal and the diet is adequate, the brain may still experience functional deficiency.
Why This Matters in Autism and Speech Delay
Multiple studies have found that a significant number of children with autism test positive for FRAA.
This can contribute to:
– Speech delay or lack of speech
– Poor understanding
– Autism symptoms like social withdrawal and repetitive behavior
– Developmental regression
– Hyperactivity and irritability
– Sleep issues
– Seizures in some cases
In simple terms, the brain may be undernourished even if nutrition seems adequate.
When Should You Suspect FRAA?
Consider testing if your child shows:
– Delayed or absent speech
– Autism spectrum disorder
– Loss of previously acquired skills
– Poor response to therapies
– Unexplained behavioral problems
– Seizures without a clear cause
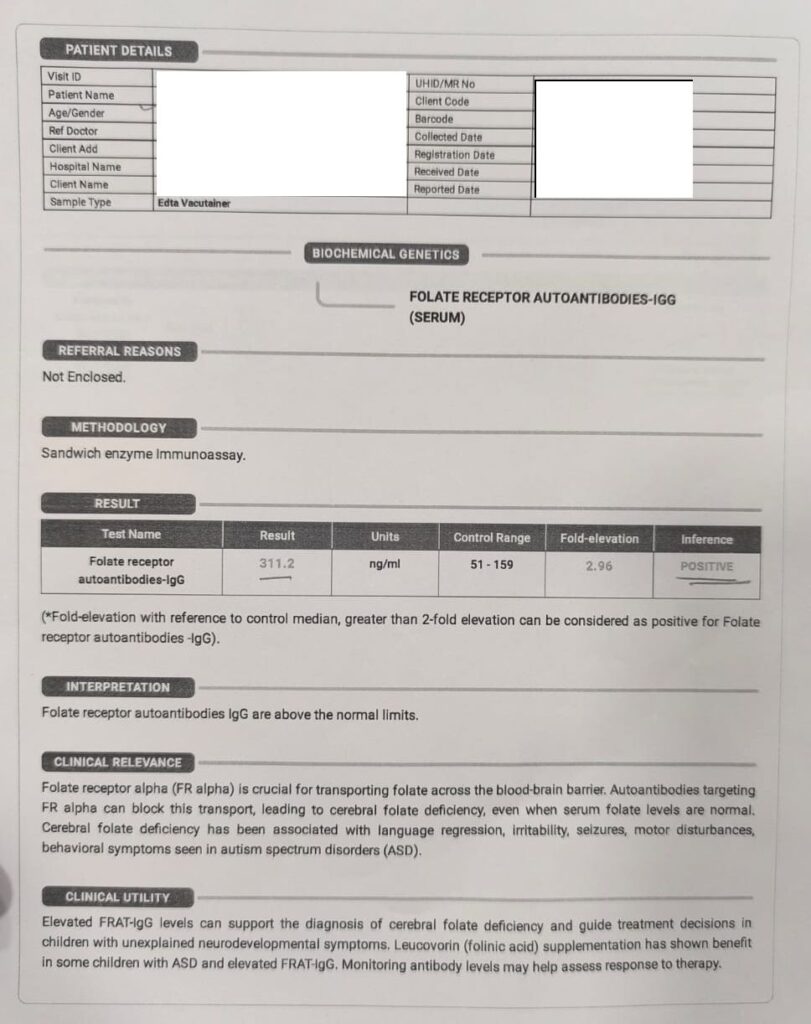
How to Test for Folate Receptor Antibodies
Test Name:
Folate Receptor Alpha Autoantibodies (FRAA)
Types of Antibodies Measured:
– Blocking antibodies
– Binding antibodies
Sample:
– Blood test
Reference Range (Important)
While exact ranges can differ, generally:
– Negative: No detectable antibodies
– Positive: Presence of blocking and/or binding antibodies
Some labs report titers (e.g., pmol/mL):
– Blocking antibody positive: > 0.2 pmol/mL, depending on the lab
– Binding antibody positive: above lab cut-off
Clinical interpretation is more important than the exact value.
Folic Acid vs. Folinic Acid — Critical Difference
This distinction is crucial.
Folic Acid (Common Supplement)
– Synthetic form
– Requires conversion in the body
– Uses the same receptor that is blocked
In cases of FRAA, folic acid may not reach the brain and can sometimes worsen the imbalance.
Folinic Acid (Leucovorin) — Correct Treatment
– Active, reduced form
– Bypasses the blocked receptor
– Enters the brain through alternate pathways
This is the treatment of choice.
What Type of Deficiency Does FRAA Cause?
It is not a dietary deficiency.
It causes:
Cerebral (Brain) Folate Deficiency
This is a functional deficiency where:
– Blood levels may be normal
– Brain levels are low
Treatment of Folate Receptor Antibodies
Note: Please do not self-medicate. Always consult your pediatrician before starting any treatment.
1. Folinic Acid (Primary Treatment)
Calcium Leucovorin (Folinic acid)
Also called:
- Leucovorin calcium
- Calcium folinate
– Common brand names: Leucorin,Biovorin,Unifolin,Leutero,Calcium Folinate etc.
– Dosage:
– Start: 0.5 mg/kg/day
– Increase to: 1–2 mg/kg/day
– Divide into 2 doses
– Duration:
– Minimum trial: 3–6 months
2. Dairy Elimination (Very Important)
Research suggests that cow’s milk proteins may trigger these antibodies.
Recommendation:
– Follow a strict dairy-free diet for 3–6 months
3. Supportive Nutrients
– Vitamin B12 (methylcobalamin is preferred)
– Omega-3 fatty acids
– Vitamin D
– Antioxidants if needed
These are only for severe or resistant cases.
Case Examples (Clinical Insights)
All the patients were under homeopathic treatment.
Case 1: Speech Delay with Autism
A 4-year-old child with:
– Minimal speech (only sounds)
– Poor eye contact
– Hyperactivity
The child tested positive for FRAA.
Treatment:
Folinic acid and dairy elimination with homeopathy
Outcome (3–4 months):
– Began forming words
– Improved attention
– Better interaction with parents
Case 2: Developmental Regression
A 3.5-year-old child who:
– Had normal early development
– Lost speech over 6 months
FRAA tested positive.
Treatment:
Folinic acid therapy with homeopathy
Outcome:
– Gradual return of speech
– Improved comprehension
– Reduced irritability
Case 3: Autism with Poor Therapy Response
A 6-year-old child:
– Diagnosed with autism
– Showed minimal improvement despite therapies
FRAA positive.
Treatment:
Folinic acid, B12, and dairy elimination and homeopathy
Outcome (6 months):
– Better communication
– Improved behavior
– Increased responsiveness
What Improvements Can Be Expected?
Not all children respond, but for those who do:
– Speech improvement
– Better eye contact
– Improved attention
– Reduced irritability
– Enhanced social interaction
Some parents report a sudden increase in speech.
Key Takeaways
– FRAA is a treatable and often missed cause.
– Blood folate levels can be misleading.
– Folinic acid, not folic acid, is essential.
– Dairy elimination can be crucial.
– Early diagnosis improves outcomes.
Final Thought
If your child has autism or speech delay and isn’t progressing as expected, consider asking:
“Is the brain getting enough folate?”
Sometimes, the problem isn’t the therapy; it’s the availability of nutrients to the brain.
FAQ Section
What is cerebral folate deficiency?
A condition where the brain has low folate levels despite normal blood tests.
Can folic acid help in autism?
Not in cases with FRAA. Folinic acid is preferred.
How long does folinic acid take to work?
Usually 1–3 months for early changes.
Is FRAA common in autism?
A significant number of children with autism may test positive.
Can I use Quatrefolic instead of Calcium folinate?
Quatrefolic is a branded form of L-methylfolate (5-MTHF) — the active form of folate. It is:
- Better absorbed than folic acid
- Useful in MTHFR polymorphisms
- Widely used in general methylation support
However, 5-MTHF (Quatrefolic) still largely depends on folate transport systems. It does not effectively bypass the receptor blockade. Hence Calcium folinate is the preferred supplement.
References
- Ramaekers VT, Rothenberg SP, Sequeira JM, et al. Autoantibodies to folate receptors in the cerebral folate deficiency syndrome. N Engl J Med. 2005;352(19):1985–1991.
- Frye RE, Sequeira JM, Quadros EV, James SJ, Rossignol DA. Cerebral folate deficiency, folate receptor alpha autoantibodies and leucovorin treatment in autism spectrum disorders: a systematic review and meta-analysis. J Pers Med. 2021;11(11):1141.
- Frye RE, Slattery J, Quadros EV. Folate receptor alpha autoantibodies in autism spectrum disorder. Mol Psychiatry. 2013;18(3):369–381.
- Frye RE, Slattery JC, Delhey L, et al. Folinic acid improves verbal communication in children with autism and language impairment: a randomized double-blind placebo-controlled trial. Mol Psychiatry. 2016;21(2):241–250.
- Ramaekers VT, Sequeira JM. Folate receptor autoimmunity and cerebral folate deficiency in low-functioning autism. Neuropediatrics. 2014;45(2):72–77.
- Quadros EV, Sequeira JM. Cellular uptake of folate: role of folate receptor alpha and reduced folate carrier. Clin Chem Lab Med. 2013;51(3):1–13.